A Distant Memory
The Past Becomes the Present

MAD
Mandibular Advancement Devices
“An Update on Mandibular Advancement Devices
for the Treatment of Obstructive Sleep Apnoea Hypoponea Syndrome”
Journal of Thoracic Medicine (2018)
An article such as this is the impetus for the extensive research into MAD devices on this website based on my traumatic history created by a mandibular splint pulling my mandible (lower jaw)
into a Class III malocclusion*to ‘recapture the temporomandibular disc’ .
*The lower jaw is in front of the upper jaw in a Class III malocclusion.
The Past
My son’s orthodontist referred me to a TMJ specialist one morning when he was examining my son and I was crying in his waiting room. Previously, equilibrating (grinding) a canine tooth during a routine dental exam had triggered a bolt of lightening through my face and initiated facial pain. Subsequent equilibration of all of my teeth by an ‘expert’ failed to resolve the pain, only increasing the intensity of the facial pain .
In addition to pulling the jaw forward, he also ‘opened my bite’ – i.e. the height of the appliance was elevated. My jaw would relax when in a reclining position and could actually go behind the upper teeth; therefore, he added a prong hanging down from the front so that my lower jaw was always pulled forward, whether upright or lying down. I could not cope and quit teaching. Physical therapy was prescribed three times a week. I later learned this TMJ specialist’ had only recently completed his first TMJ course and I was among one of his first TMJ patients.
I was already seeing a chiropractor; one of the pastors at my church had referred me to his long-time chiropractor who had done wonders for my low back after two back surgeries had failed to resolve pain from a herniated disc and subsequent spinal fusion. This trusted doctor was horrified at what was happening to my neck and cervical spine as the dental appliance pulled my lower jaw forward. An unexpected high-velocity thrust to my head and neck was devastating; the left side of my head felt like it collapsed inward at a diagonal angle. I was in such shock, I left without saying anything; I was very scared and never went back.
I started counseling. The therapist asked me to identify my greatest fear. I clearly remember the question, my answer and his response. “I’m afraid of the pressure that’s building up in my head from this splint and that my head will implode.”
His response said it all: he simply stared at me, was speechless and held my hand.
Yesterday | 1978-1981
The 70’s treatment for TMD of ‘recapturing the temporomandibular disc’ by using a mandibular appliance has changed radically. By 2000, this procedure for treating Temporomandibular Dysfunction (TMJ or TMD)) had been discontinued.
In 1999, I had an appointment with the dentist who wrote the TMJ ICD (international classification
of codes). He offered a profuse apology for his profession for their treatment of me and stated that ‘recapturing the disc’ by pulling the mandible (lower jaw) into a Class III malocclusion was no longer done.
It appears, however, that similar appliance applications are now used for a different diagnosis …
Obstructive Sleep Apnea
and Snoring!
There is general non-recognition
of the potential structural complications that can happen from
mandibular advancement.
Four months later, I became the ‘star’ pupil in a TMJ dental symposium.
My case was presented and my name became notorious in dental circles.
The recommendation to remove the lower appliance and use a maxillary split was unanimous.
I changed dentists. The abrupt shift in jaw position and appliance
left me unable to lay down without severe pain; therefore, the dentist performed daily
anesthetic injections in the palate so that I could lay down to sleep.
At this point, a psychiatrist joined my team of doctors, the same psychiatrist who was treating my Mother. His sister happened to be a dentist; thus, he seemed a most appropriate choice.
He prescribed heavy doses of valium.
It was 1978. For more detail, read Basket Case.
In May 2025, I relayed this history to my San Jose dentist and Phoenix oral surgeon.
They were both horrified.
“Oh my God. This is irreparable”, exclaimed my dentist.
“This is what we’re trying to fix now,” I stated.
The oral surgeon was speechless when he learned the name of the dentist
who had treated my alleged “TMJ” in 1978 with this procedure.
He has known him since that time.
The Present
There is currently an astounding number of MAD devices
used to treat OSA [obstructive sleep apnea].
Rather than recapturing the TM disc,
these devices are designed to “open the airway”.
The mandible (lower jaw), skull base and cervical spine are a different anatomical issue than the maxillary midline suture with maxillary (upper jaw) devices.
In a 2018 orthodontic journal article,
the issue of potential complications is addressed:
Side Effects of Mandibular Advancement Splints
for the Treatment of Snoring and Obstructive Sleep Apnea:
A Systematic Review
“Occlusal side effects or development of pain and/or functional impairment of the temporomandibular complex are potential reasons for poor compliance or abandonment of mandibular advancement device treatment for snoring and obstructive sleep apnea.”
Conclusion
Long-term assessments of adverse effects of MAS (mandibular advancement splints) therapy with larger study samples and recruitment
of homogenous patient population are still required.
Today | 2025
Both of the references pulled from the internet on this webpage are 2018 articles. One is more hopeful than the other.
There is general non-recognition
of the potential structural complications that can happen from
mandibular advancement.
Dental History
Years of Discovery
1- 1977-1981
Dental trauma with equilibration (grinding of teeth) triggering orofacial pain followed by TMJ misdiagnosis and mismanagement with MAD (mandibular advancement device*) as well as multiple maxillary dental devices.
2- 1996
Orthodontic injury causing palate to shift with the left pterygoid hamular process dropping down into the palate, triggering fluid in oropharynx within thirty minutes of the procedure and later alternating with an ‘icepick sharpness’ symptom.
3- 1998 —-> 1971
Hamular Process resection to reduce the ‘sharp’ sensation. Symptoms remained. Discovery of an Intubation injury during a sinus surgery (1971) with resulting necrosis (dead bone) in the hamular process region of the palate – up and behind the third molar.
4- 1999 – 2023
No answers and no diagnosis

AND yet another piece of the orofacial puzzle unravels –
from the Tensor Veli Palitini
to the Temporalis Tendon
Tensor
tensor veli palitini
My March discovery of the ‘inferior’ attachment of Raphe in the retromolar area adjacent to the Temporalis Tendon triggered innumerable thoughts, swirling and spinning into an ‘aha’ moment of insight – or illusion?
The interaction of the swallow and the tongue at this critical junction (Hamulus / Tensor Veli Palitini / Torus Tubarius / Tubarial Salivary Gland) with the Pterygomadibular Raphe and its attachments has been a missing link in my complex history.
What is the significance of the Temporalis Tendon?
The Temporalis Tendon is a downstairs ‘next-door neighbor’ to Raphe’s anchor behind the third molar (retromolar trigone area). What happens to Raphe’s friend Tempo (temporalis tendon) at the inferior (bottom) end with Tensor (tensor veli palitini) ‘flopping around‘ in the tissue upstairs?
The tissue in the oropharynx has been ‘assaulted’ by my dentist since October. My mandibular device (NOT a mandibular advancement device) provokes occlusal shifting which affects the tissue. This mandibular appliance has gradually provided occlusal stability which was destroyed in the 1977; attempts to restore this stability have failed. In April, my San Jose dentist confirmed the occlusion had stabilized. “Don’t feel like you have to make appointments for occlusal adjustments every month now; I’ll be glad, however, to see you when you’re in Santa Cruz.”
Is it coincidence, or cause and effect, that the ‘constrictor muscle’ spasm – initially discovered over a year ago by all three doctors – ENT and both osteopaths – has shifted? Hello Tempo (temporalis tendon).
In March, I was wondering if the Temporalis Tendon had suffered consequences from not only Raphe’s orthodontic injury in 1996 but also the TMJ dental mandibular trauma in 1978?
The months of April and May are providing answers.
Tempo
temporalis tendon
The dental equilibration destroying my natural teeth and occlusion and then pulling the jaw forward
created havoc and years of dental and orthodontic confusion and pain into the NOW – 2025.
What was done then is not done now…. for TMJ.
HOWEVER, the jaw is still being pulled forward
with MAD appliances today for a different diagnosis
along with a host of other devices.
Practitioners do not seem to understand that the head
is attached to the body and what is done to the jaw, oropharynx and skull base can and does affect
structure and function.
Oral Protraction Head Gear, Palatal Expanders, Protraction Facemasks,
Reverse Pull Headgear, Orthodontic Facemasks
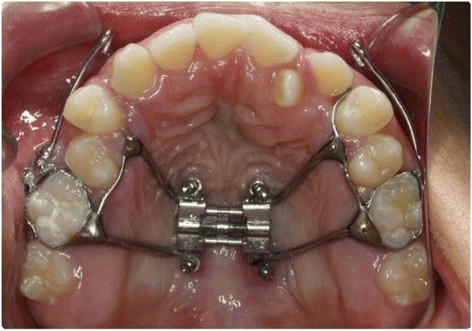
Micro-implant-supported hyrax with facemask
Source: Research Gate

The head is attached to a body.
And along with the hip and the shoulder,
the jaw (temporomandibular joint) is one of the most movable parts in the body.