Osteopathy Meets Orthodontics
The intersection of Orthodontics
with the Cranial Osteopathic perspective
is critical and revolutionary!!

Do you know someone who has worn braces
and their teeth moved back after the braces were removed?
Why are retainers necessary once teeth are ‘straight?”
Two orthodontic perspectives in practice.
… a Clash of Contradiction?
– Maxillary (upper jaw) appliances crossing the midline,
several crossing the palate and one behind the upper front teeth.
– Mandibular (lower jaw) appliances
one having the potential to lock the lower jaw
and the other having significant structural ramifications for the jaw joint and the neck.
– Crossing the maxillary midline suture with an upper splint –
– Locking the mandible with a lower splint –
– Creating an anterior forward jaw position
with a lower splint –
And therein lies my experience, insight and awareness
and leads me to
WONDERING and QUESTIONING
BUYER BEWARE
Our aim is to educate.
There is a multitude of oral devices on the market
…for sleep apnea, swallowing, TMJ, malocclusions and aesthetics.
Awareness and the ability to ask relevant questions for your specific circumstance
is of paramount importance in this dental world of numerous options.
There are two different perspectives that collide in this dental arena,
underscoring the relevance and realization of treatment potentials,
both positive and negative.
Is there a ‘missing piece’ that could have major implications
for the ‘negative’ experiences, some of which end up in lawsuits?
Are these ‘disaster’ cases caused by the device, the practitioner,
or lack of awareness and/or non-acceptance of another perspective?
Welcome to the
Cranial Osteopathic Orientation.
Raise your awareness of orthodontic practices and potential repercussions.
Learn how Cranial Osteopathy enters this Orthodontic, Orthopedic, Orthotropic® scenario.
..other than they all begin with the letter O!
This discussion presents TWO different perspectives… two different orientations
…with common goals?
Orthodontic Orthopedics
[dentofacial, craniofacial, epigenetic, orofacial, craniomandibular]
and Cranial Osteopathic
[facial development, orthotropic]
Screws? Braces? Light wire, Heavy wire?
Palatal Expansion, Slow or Rapid? Surgery or Oral appliance?
Arch Development? Pre-Orthodontic? Unilateral BiteBlock®?
It’s a Jungle out there!
Learn the Lingo:
Ask an intelligent question, know your orthodontic options and
discover the expertise or the ignorance of the practitioner !
Orthodontics specifically deals with the misalignment of teeth, commonly referred to as malocclusion. Orthodontic appliances like braces or aligners are used to correct misaligned teeth, overbites and underbites, gapped, crooked and crowded teeth, and other dental structure-related issues so a patient can have a better bite, healthier teeth and a more beautiful smile.
Orthopedics – a plethora of terminology enters the picture – and all of these ‘orthopedics’ work to correct all of the “teeth: issues mentioned above. Furthermore, orthodontic orthopedics can treat and manage jaw positions related to the face and skull by controlling the growth of facial bones as well as the jaw. This is best done during the childhood growth spurt when the bones are in ‘a rapid growing condition.’ A proper bite and smile can be achieved in children with the help of appliances; on the other hand, surgery may be required for adults.
Orthotropics® – developed in 1966, treats the face rather than just the teeth with a focus on forward growth of the upper (maxilla) and lower (mandible) jaws. Facial Orthotropics® refers to the growth and guidance of the face. Why are teeth crooked? Orthotropists believe that malocclusiond (crooked teeth) are a biological issue of growth and development; removable, widening appliances are utilized to widen the palate and make room for the tongue to correct the underlying causation before orthodontic intervention with braces.
Currently, the adult population wearing braces, invisalign, and retainers
is almost as commonplace as grade school children and teenagers!
Straightening teeth and perfecting the bite (occlusion) is the primary goal;
and retainers have become as familiar as the toothbrush.
The dentist has become a ‘go-to’ doctor for
breathing problems, snoring, sleep apnea, facial neuralgias,
and TMD (temporomandibular joint dysfunction).
In addition, the dentist serves as a secondary ‘aesthetician’,
the creator of the ‘perfect smile with shining white teeth’.
And for the older generation with bone loss in their “aging adult” face,
hope for a more ‘youthful’ appearance.
Today, the trend is not only a beautiful smile but also a perfect face –
widening the palate (expanding the maxilla) helps achieve this goal, even in an adult!
And the world-wide “Mewing” craze
must be included in this palate expansion phenomenon.
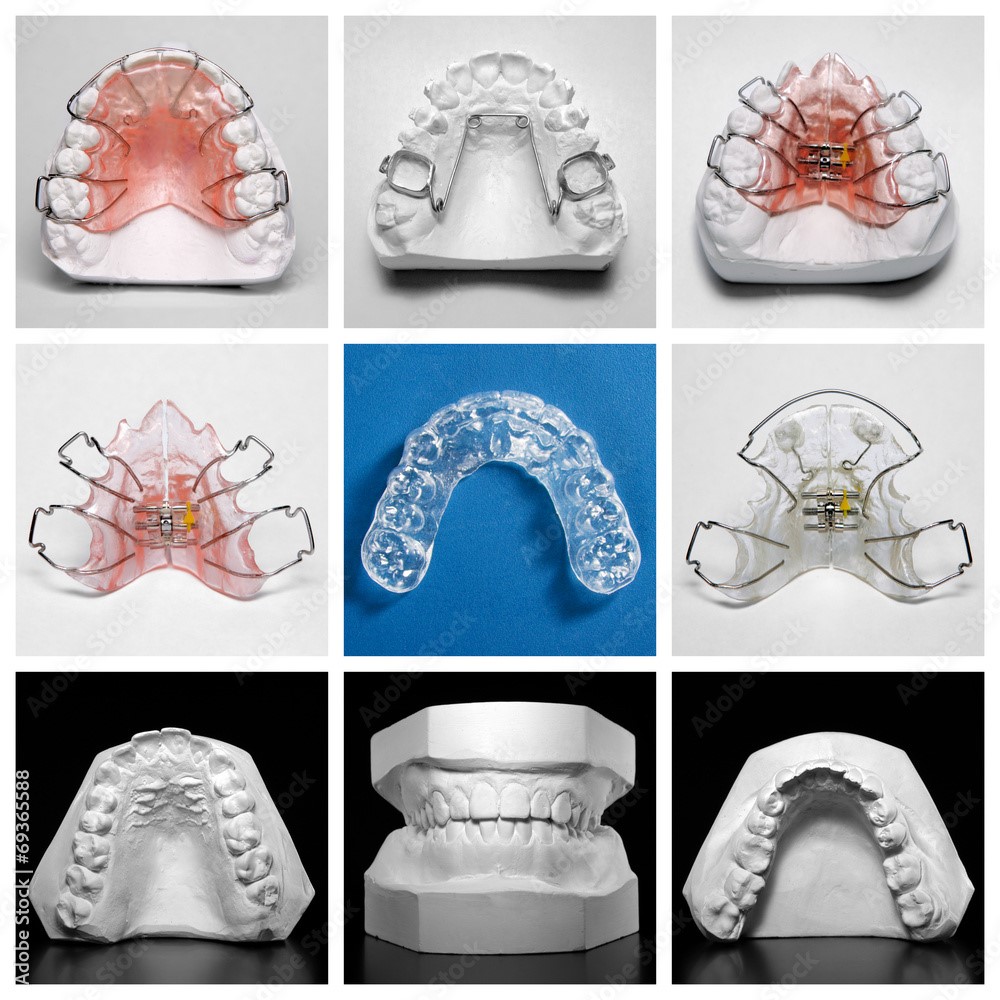
Maxillary (upper jaw) Appliances*
Mandibular (lower jaw) Appliances*
1- The ALF appliance (1982) utilizes an adjustable light wire force for the dental appliance
to create a functional swallow
in conjunction with the inherent motion of the body to ‘balance the mechanism’
(osteopathic ‘whole body’ orientation)
in preparation for potential orthodontic intervention.
The last phase of the ALF approach
is straightening the teeth.
2- The Homeoblock™ uses a light force with a screw
to widen the palate on the maxilla (upper jaw)
and has Unilateral Biteblock Technology®.
3- Orthotropics® and Facial Development
The BioBloc – maxillary expansion
The MyoBrace® – pre-orthodontic treatment
4 – The Crozat – arch development
6- The Vivos DNA appliance
(daytime nighttime appliance).
Used for sleep apnea and TMJ disorder.
Two different orientations…
both with common goals –
better breathing.
1 – The POD™ (2019), a mandibular (lower jaw) appliance for better breathing, bruxism and TMJ,
has Unilateral Biteblock Technology®.
2 – There are innumerable MAD (Mandibular Advancement Devices) for sleep apnea
as well as for clenching and grinding.
*this list is not comprehensive
The Early 1980’s
Forty years ago
my dental education
soared with unfortunate
TMD and dental splint experiences.
My adventures within the dental community
and falling into the world
of the Cranial Osteopath
vividly illustrate the juxtaposition of
dental and orthodontic practices with osteopathic perspectives.
These issues are
extremely relevant today,
for both children and adults.
Dental orthopedics was evolving during the era that my children underwent orthodontic care – the early 1980’s. This was also the years when equilibration (grinding teeth) and dental appliances were unsuccessfully used in treating my temporomandibular joint dysfunction (TMD). My awareness as a parent taking children to an orthodontist had grown by leaps and bounds because of my unfortunate experiences in the dental community with TMJ and equilibration: I was able to ask educated, uncomfortable questions.
The first orthodontist we visited recommended headgear. My question “What are you doing to their temporomandibular joint with this restriction?” met with an unacceptable response of “I don’t know“. This compelled me to seek another practitioner.
I found an orthodontist who utilized a non-traditional approach – “craniofacial orthopedics” – rather than the traditional headgear. He had changed his practice because of his awareness of the osteopathic cranial orientation and implications for orthodontics. When I questioned this second orthodontist what was happening to their neck and cervical spine while he was repositioning their lower jaw with an orthopedic device, his response was, “I don’t know.”
My suggestion that they undergo cranial osteopathic treatment after each splint adjustment was supported one hundred percent: “I wish all of my parents would do this.” Thus, my children underwent craniofacial orthopedics in conjunction with osteopathic care during their “growth spurt” orthodontic years.
Today, I realize how fortunate that a ‘craniofacial orthodontist’ was located in our immediate neighborhood – not a common occurrence during this era. .
Maxillary (upper jaw) Appliances
The ALF Apppliance
My children’s orthodontist wasn’t the only dental professional becoming aware of the
Osteopathic orientation in the dental and orthodontic world.
Meet a California dentist from this same era
…who observed his patients under osteopathic care in conjunction with his dentistry,
…and who not only changed his practice but also was curious and creative.
The ALF appliance was fashioned by Darick Nordstrom, DDS in 1982.
The ALF Appliance is a non-traditional orthodontic approach.
This approach recognizes the teeth as part of the jaw and skull attached to the body
and thereby considers the structural implications of orthodontics
This different perspective is known as Advanced (Alternative) Light Force.
This ‘lightwire’, ‘lightweight’ “cranial friendly” appliance, designed by Darick Nordstrom DDS.
is an integrated, collaborative whole body approach for treating facial growth and developmental dysfunction.
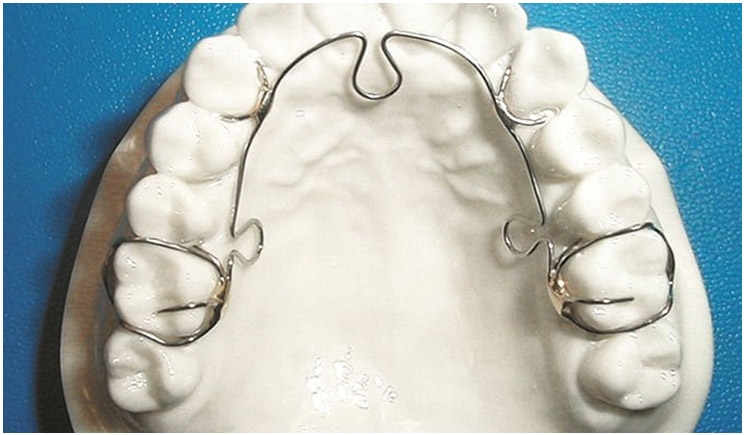
The ALF Approach (Tasha Turzo, DO) is a thorough compendium of this perspective. Note that the appliance crosses the midline with a ‘horseshoe’ bend behind the teeth rather than the palate. The appliance is made from Elgiloy® wire, one of the most versatile alloys used in orthodontics today, The unique and essential goal of the ALF approach is to augment and stimulate inherent motion of the craniofacial complex.
The ALF perspective as a whole body approach recognizes the interaction between the jaw and skull base
with the cervical spine, thoracic cage and pelvis
as well as the significance of tongue placement for correct swallowing and breathing.
A team approach involves dentist, osteopath and perhaps a myofunctional therapist.
Craniofacial Osteopathic Orthopedics is
more descriptive of this cranial, whole body orthodontic approach.
Facial Change with Fascial Integrity
Tongue to Toe
The Homeoblock™

The Homeoblock™, created by Theodore Belfor, DDS around 2005, is used to remodel the maxilla (upper jaw) to provide proper jaw positioning and more room for the tongue in both children and adults. Physiologic change from light force stimulates bone growth and changes in the facial bone structure.
This device is the ‘future’ of dental aesthetics: arch, jaw, and facial development. Underdevelopment of the dental arch can lead to temporomandibular joint disorders as well as sleep and breathing disorders. Neuromuscular dentistry and the health of the airway are major considerations beyond teeth.
Intra-oral appliances are not new. How is the HomeoBlock different?
There is an acrylic bite block on one side only. The appliance does not touch soft tissue. Long arm flap springs come in contact with the teeth. The appliance is worn from six – ten hours overnight. The patient expands the appliance with an expansion screw at .25 mm for each turn – the width of the mid-palatine suture; this rate of expansion is physiologic.
When the patient swallows, the teeth come in contact with the Unilateral Biteblock Technology®, negative pressure on the mid-palatine suture begins the process of bone remodeling at the suture. When swallowing, the tongue pushes up against the acrylic plate which flexes. Saliva pulls under the acrylic plate. and when the pressure is relieved, negative pressure is thereby exerted at the suture. Minor forces are exerted on the teeth with this pressure change, thereby sending receptors to the periodontal membranes of the teeth. These cascading series of events pass through the cell membrane nucleus of the osteocyte, as outlined by Dr. Melvin Moss, head of the anatomy and cell biology at Columbia University and creator of the Functional Matrix Hypothesis.
(NAAFO) North American Association of Facial Orthotrophics has merged with the
AAGO (Academy of Airway and Gnathologic Orthopedics)
Biobloc or MyoBrace with Orthotropics®
or Crozat appliance with Gnathologic Orthopedics?
These three appliances utilize function (chewing, swallowing and rest oral posture)
in combination with light forces on the teeth to create changes in the underlying bone.
All three devices
– Preserve the patient’s natural dentition, and
– Employ non-extraction orthopedic techniques
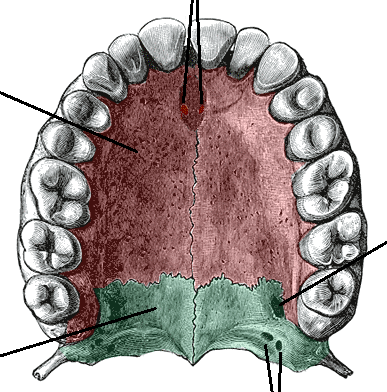
All three cross the maxillary (midline) suture of the palate.
This is a major consideration in the
Orofacial Osteopathic Perspective that recognizes cranial rhythm
and the inherent subtle motion that exists at the maxillary suture as the tongue
gently massages this palatal suture with a functional swallow 2000 times or more a day.
The ALF appliance is the ONLY orthodontic device that does NOT cross the midline.

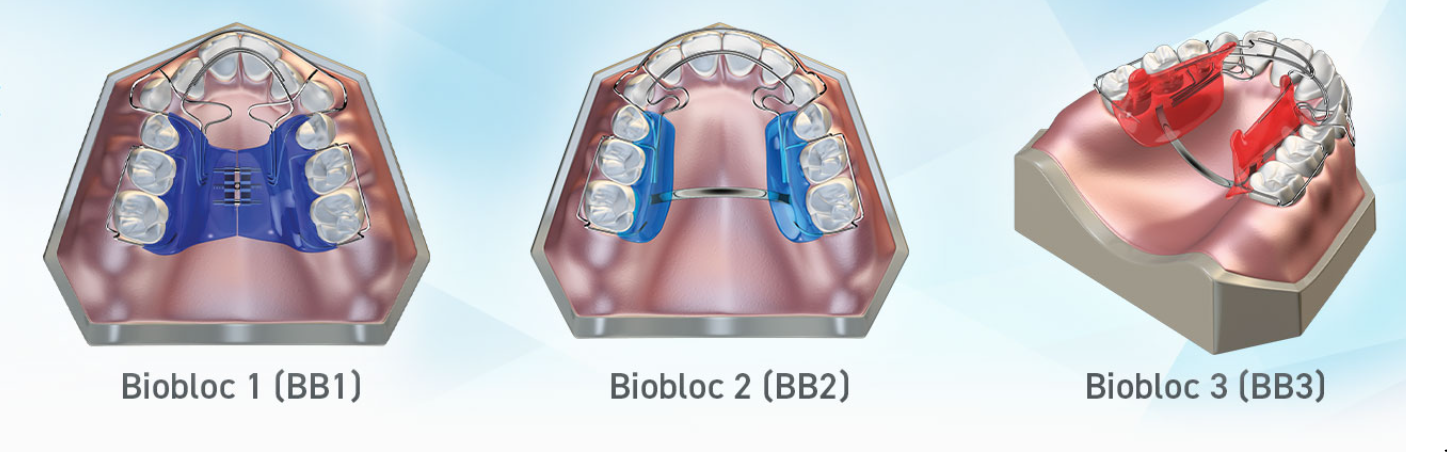
The Biobloc is an Orthotropic® product. Biobloc Orthotropics® is a series of removable orthodontic appliances and brackets that are part of the Orthotropics® technique, which is used to guide the growth of the upper and lower jaws.
The Orthotropics® technique was developed in 1966.

A preventative, pre-orthodontic treatment designed to deal with incorrect myofunctional habits by teaching patients to breathe through their nose, rest the tongue correctly in the roof of the mouth, swallow correctly and continue widening the jaws so they grow to their full and proper size.

The Crozat objective is
Arch Development,
different from the more prevalent idea of transverse maxillary expansion.
Comparison and discussion of palate expanders,
including the Crozat and ALF.
NOTE: No mention has been made regarding the maxillary midline suture
and the effects of a screw (Schwartz, Homeoblock, DNA) or crossing the midline (Crozat) on the maxillary suture.
The focus is on the mechanics of expanders in the mouth and how to attain a forward growth of the face.
The effects of changes in the orofacial complex/mouth on the whole body are ignored.
When the mechanics of the jaw joint/palate are altered,
it is critical that the effects on the sacroiliac joint and pelvis need to be addressed.
The Orofacial-Pelvic Connection
discusses this reciprocal ‘balance’ of the body.
The potential impact of this ‘head back’ connection follows this discussion
with my personal ‘orofacial-pelvic’ narratives:
The Prognosis Protest, The Basket Case and Serendipity and Providence (1977-1981)
as well as by a later Orthodontic Ordeal and Detour in California in 1993.
Discover the potential ‘adverse repercussions’ that can occur
when this body-balance’ between the sacroiliac joint and orofacial complex is changed and restricted
as well as the potential for positive change, evident in the palate at the maxillary suture,
when cranial osteopathic treatment intervenes
The Vivos DNA Appliance
Another palate expander with a screw crossing the midline.
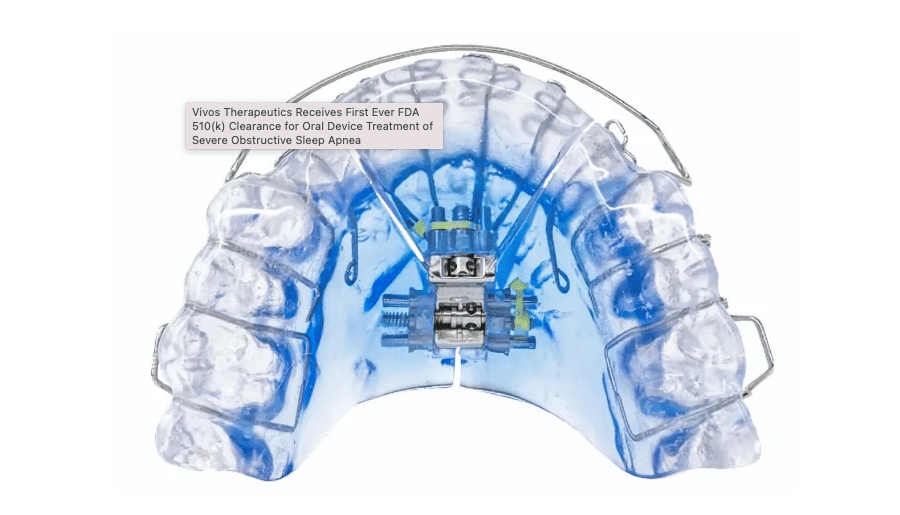
The DNA appliance is a removable appliance for the mouth that safely,
gradually and painlessly stretches the upper arches of the teeth.
This allows more room for the tongue without blocking the airway, causing sleep apnea.
Vivos has received the first FDA 510(k) clearance for Oral Device Treatment of OSA
(obstructive sleep apnea) in adults, 18 years of age and older.
Mandibular (lower jaw) Appliances
The POD™ Preventative Oral Device
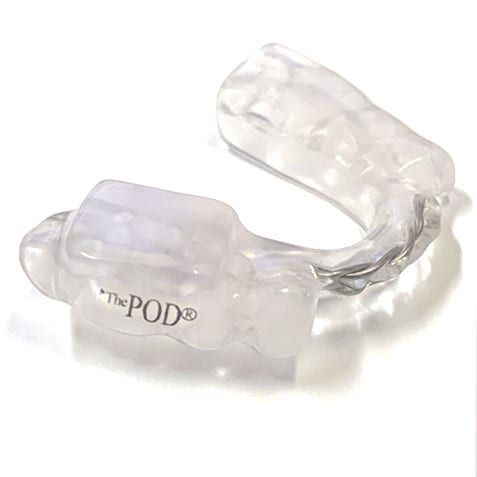
The POD™ is an intraoral mandibular (lower jaw) device designed to aid in treating clenching grinding (Bruxism) and TMJ (temporomandibular joint). Protecting the teeth from Bruxism can help with headaches, musculoskeletal pain and TMJ.
This device, featuring Unilateral Biteblock Technology®, can reduce muscle tension and allows for better breathing during sleep. The POD™ assists myofunctional therapy for better tongue posture to create proper breathing: the tongue is placed at the roof of the mouth for swallowing and the body thereby creates better breathing habits over time.
The Unilateral BiteBlock Technology® allows for more room for the tongue, which is free to come forward for better breathing during sleep in contrast to a flat plane occlusal night guard which inhibits the tongue from coming forward.
The POD™ device is not one of the many Mandibular Advancement Devices (MAD) that position the lower jaw in an anterior/forward position.
MAD
Mandibular Advancement Devices
This 80’s treatment in TMD of ‘recapturing the TMJ disc ‘by using a mandibular advancement device has changed radically.
By 2000, this procedure for treating
Temporomandibular Dysfunction
had been discontinued.
It appears, however, that similar appliance applications are now used for a different diagnosis …Sleep Apnea?
There is general non-recognition of the potential
structural complications that can happen
from mandibular advancement.

There is currently an astounding number of MAD devices used to treat OSA [obstructive sleep apnea].
Rather than recapturing the TM disc, these devices are designed to “open the airway”.
The mandible (lower jaw), skull base and cervical spine are a
different anatomical issue than the maxillary midline suture.
In a 2018 orthodontic journal article, the issue of potential complications is addressed:
Side Effects of Mandibular Advancement Splints
for the Treatment of Snoring and Obstructive Sleep Apnea:
A Systematic Review
“Occlusal side effects or development of pain and/or functional impairment of the temporomandibular complex
are potential reasons for poor compliance or abandonment of mandibular advancement device treatment
for snoring and obstructive sleep apnea.”
Conclusion
Long-term assessments of adverse effects of MAS (mandibular advancement splints) therapy
with larger study samples and recruitment of homogenous patient population are still required.
My case serves to
validate and confirm
– Validity of the cranial osteopathic perspective.
– Confirmation of the results of treatment with health care practitioners trained
in the cranial osteopathic orientation.

My case serves
to expose and reveal
– Orthopedic dental devices crossing the midline and potential restriction of cranial motion.
– Use of dental splints or orthodontic procedures in the presence of (unknown) necrotic bone.
– Open bite appliance potential adverse effects
for treatment of TMD (temporomandibular joint dysfunction).
The potential adverse effects of Mandibular Advancement Devices (MAD),
previously used to treat TMJ by ‘recapturing the disc’ and now being used for sleep apnea.
EXPERIENCE
…the teacher of life that provides food for thought to ‘chew’ on
– literally and figuratively.
Walking through a looking glass, falling down a rabbit hole,
discovering an uncommon path, seeing a rainbow,
and uncovering a pot of gold.
…in the hands of a cranial osteopath
AWARENESS
For the Professional
Orthodontic and Dental Awareness
Patient Specific Treatment
For the Patient
Patient Education and Awareness
Freedom of Choice
In hindsight, pre-existing ‘extenuating circumstances’ were most likely
the invisible and silent infrastructure of the dental repercussions and overall deterioration.
My unusual case of known and unknown pre-existing conditions was most uncommon
and emphasizes the relevance of medical history.
an unrecognized intubation injury to the palate in conjunction with anesthetic awareness experience
a spinal fusion in the lower back
My hope is to raise awareness
of the Unconventional, of the Non-traditional.
– and of POTENTIAL
for the benefit of the “Uncommon Patient”.
….maybe a pot of gold for another patient
..or maybe something to ‘chew’ on for a dentist or orthodontist!
WONDERING and STORYTELLING
in respect of and for the Uncommon Patient
I wonder if the little ‘horseshoe turns’ in the ALF appliance
is what allows for movement and thus palatal motion with the swallow?
… thus, no restriction of cranial motion, but rather,
as stated by the creator of the appliance as well as osteopathic physicians,
enhancement of cranial motion.
I wonder if the Homeoblock™, by not touching the soft tissue of the palate
and utilizing a spring-loaded action activated by swallowing,
allows for cranial motion
even though it crosses the midline and expands the dental arch with a screw?
I wonder if both the ALF and the Homeoblock™allow for
inherent motion at the maxillary midline,
…the heart of the osteopathic orientation?
I wonder about an open bite position
created by the Unilateral Biteblock Technology®
and utilized in both the Homeoblock™ and the POD™ devices.
What happens to the skull base and spine when the teeth
begin to shift and occlude due to an open bite?
I wonder if the Mandibular Advancement Devices [MAD]
currently in use today, have the potential
for the structural harm that happened in my case?
I wonder how many patients in the adult orthodontic population
with root canals or dental implants
are hypercoagulable, which increases the probability of
having an undetected bone infection*?
And, thus what are the ramifications for
expanding palatal bone at the maxillary suture,
or possible structural complications inherent in mandibular advancement,
or for any orthodontic procedure?
Mandibular Advancement | 1978
The creator of CPT codes for TMD (temporomandibular joint dysfunction) apologized, on behalf of ‘his profession’, for the mismanagement of my TMD case in 1978 – the ‘recapture the TM disc’ treatment with mandibular advancement into a Class III malocclusion..
It was 1999 – twenty years later.
This dentist informed me that I had been placed in a 24-hour whiplash position for five months. The fact that I had a spinal fusion in the lower back that was an inch too anterior compounded the structural nightmare that went ‘unrecognized’ by the dental community. Dismissal from a dental practice, being labeled a ‘psychiatric case’…the lack of understanding and unprofessional behavior in several instances was almost as detrimental as the splint treatment itself.
The structural stress on my head, neck and back rendered me nonfunctional – and thus I became the dental Basket Case of 1978 in Phoenix, Arizona. It was after this initial structural mandibular insult to my body, that four maxillary appliances rapidly increased my deterioration.
1979 – 1980
Maxillary Appliances
The dental appliances (four in two years) that had rendered me nonfunctional
had unmistakably restricted palatal motion, creating whole-body repercussions:
not only in my jaw and face but also in my neck, back and legs –
my body was adversely affected in totality.
This response was ‘unknown’ and ‘bizarre’
in my dental community.
The cranial osteopath not only recognized the detrimental whole-body response
to the dental appliances
but also was able to help my body recover from the unidentified and unintentional damage created by the dental community in the name of splint therapy.
Crossing the midline
with a fixed appliance
can interfere with
cranial motion
which in turn affects
physiologic and
structural functioning
of the entire body.
My early dental adventures
during 1978 – 1980 served as
preparation for my entrance
into the world of the cranial osteopath.
Per the Osteopath’s request – the hard acrylic maxillary dental appliance with gold prongs over the teeth to prevent all motion, was split at the midline. This allowed the inherent cranial motion at the midline of the palate to be restored.
Within six weeks of this splint adjustment in conjunction with osteopathic treatment,
the gap at the midline of the appliance expanded approximately nine millimeters.
Positive change in six weeks
after four years of dental mayhem!
In the eyes of the dentist, the appliance was no longer ‘functional’.
However, in the osteopathic world, the patient was more functional!
The dentist said he was unable to proceed with treatment with a midline split in an appliance and dismissed me.
And I was unwilling to continue dental treatment,
fully aware that my problem was much larger than my jaw and chasing ‘perfect occlusion’.
It was now 1981.
Orofacial – Pelvic Connection | 1994
In the mid 90’s, I was yet again in the world of dentistry attempting to restore my bite (occlusal stability), this time as a patient of an orthodontist who refused to use dental splints for balancing occlusion and treating TMD. Working from the osteopathic cranial perspective of NOT crossing the midline, acrylic pivots were bonded to a lower molar on one side. Thus, the bite was opened on one side during this ‘pivot process’ in order to manipulate the temporomandibular joint functionality and thus adjust the occlusion to “stabilize the jaw joint”.
My bite would rapidly occlude (teeth coming together to create a bite) with this procedure; in the orthodontic world, the rapidity was surprising. I was one of many patients treated with this ‘Open Bite’ procedure for ‘manipulating’ the jaw joint. This treatment eventually precipitated an extrusion of the molars which resulted in a radical adjustment of my occlusion – the pivots were ground down. Within ten days, my neck and back violently reacted. I was on crutches and in and out of a wheel chair for months . The immobility at my spinal fusion at L5-S1 could not handle the repercussions of this occlusal/jaw joint change – the orofacial-pelvic connection personified.
Bone Injury and Hypercoagulation | 1998
My bite was ‘restored’ by a colleague of the orthodontist. When I was able to walk again without crutches, the orthodontist ‘fine-tuned’ the occlusion and ground an upper left canine tooth. This small occlusal adjustment on June 4, 1996 at 10:30 am resulted in yet another dental disaster within thirty minutes of the procedure.
The left hamular process in the palate shifted down into the roof of my mouth, nor only palpable but visible.
Two years later, I was referred to a research oral surgeon specializing in osteonecrosis of the jaw. He uncovered the source of this ‘uncommon’ response through initial lab testing for hypercoagulation and later confirmed during a surgical biopsy: Necrotic (dead) bone in the palate caused by an intubation injury during sinus surgery (1972). The intubation bruising impaired microcirculation to the bone, causing slow bone deterioration in the hamular process area of the palate.
My closet shelf houses a collection of more than thirty CT and MRI scans;
not one of them indicated the necrotic (dead) bone uncovered during this surgical biopsy in 1998.
StoryTelling
For a detailed journey into medical mayhem within the dental and orthodontic communities,
the following stories below reveal themselves
to be the source of the Wonderings as well as
provide validation and credibility of the Cranial Osteopathic Orientation.
The interface of Osteopathy and Orthodontics
is a natural place to observe the body in motion.
Most Orthodontics and Dentofacial Orthopedics inherently have
unrecognized adverse potentials and limited understanding of the totality of treatment.
I wonder if we are more Common than Uncommon?
I wonder how many dentists and orthodontists utilizing appliances
are aware of this ‘other perspective’ in the world of the cranial Osteopath
for those patients who exhibit “unknown” repercussions?
I wonder how many ‘disaster’ cases in this field are due to ignorance or
dismissing the knowledge and expertise of Osteopathy in the Cranial Field?
And I wonder how many of these ‘disasters’
can be treated or could have been avoided with more awareness?
Why, What, and How ?
Why is a spinal fusion in the lower back and a dental splint on the upper teeth
elements of A Perfect Storm in the world of the Cranial Osteopath?
Read A Perfect Storm and join me on
The Road Less Traveled

Read The Sound of Silence
and follow my story
into the Invisible
…The Before

Read The Prognosis Protest
and follow my story
of two unsuccessful back surgeries
….after the Silence

Read The Basket Case
and follow my story of
dental splints that crossed the midline
of both upper and lower jaws*.
[*pulling the lower jaw into a Class 3 malocclusion
to ‘recapture the TM (jaw joint) disc’]

Read
Serendipity and Providence
and follow my story as I
wandered onto
‘The Road Less Traveled’
with cranial Osteopathic treatment.

Read ‘Cold Turkey’ Potency
and follow my story of
splint treatment recovery with medication withdrawal
….and the surprising benefit of osteopathic cranial treatment.

The Next Twenty Years

The “Beyond”
of the Unknown
20 years later – in 1998 –
Discoveries and Confirmations
of the Why, the How, and the What
…in the office of an oral surgeon.