My name is Raphe, a nickname for Pterygomandibular Raphe. I am not a pterodactyl dinosaur – I am a ligament. You may recognize me from our initial meeting in December as I appeared from the Unknown; more recently in February, I became very vocal.
I’m back again…. and introducing more surprising discoveries with several friends!
Tensor Tensor Veli Palitini
Torus Torus Tubarius
RAPHE
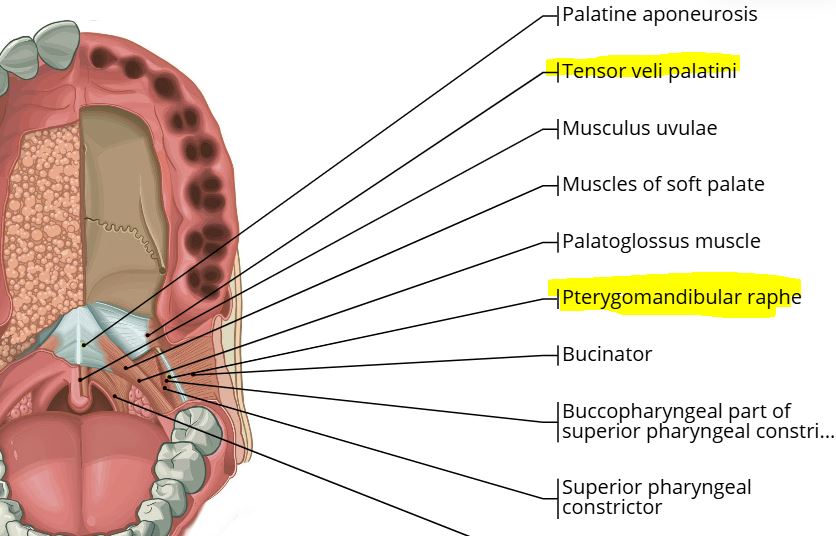
Pterygomandibular Raphe
Tubby Tubarial Salivary Gland
Tempo Temporalis Tendon
A Tissue Issue with Tensor (Veli Palitini)
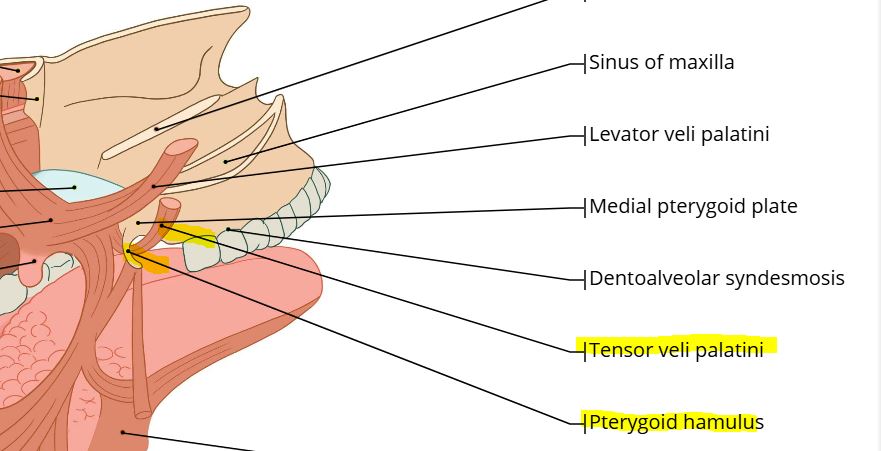
As mentioned before, the ligament Raphe (pterygomandibular raphe) has both a superior (high) and an inferior (low) attachment. And his superior attachment at the pterygoid hamulus no longer serves as his anchor. His stability (the hamular process) was traumatized by an orthodontic procedure in 1996 and the consequences confirmed during an oral surgery in 1998.
His muscle friend ‘Tensor’ most certainly was affected since the tensor veli palitini wraps around the hamulus. The hamular process had disintegrated at the touch of my oral surgeon’s pinky finger. His comment after surgery remains etched in my memory forever:
“I didn’t even have to snap the hook on the hamulus… it dissolved at my touch. Your hypercoagulation genetics compromised microcirculation to the bone from your 1971 intubation injury. Bruising of the bone impaired healing and, after 25 years, the bone is dead.
Tensor plays three important roles:
Action:Tenses the soft palate
Related function:Opens the Eustachian tube
When activated:During swallowing or yawning
Meet Tensor
Recently, my oral surgeon commented that Tensor was probably ‘flopping around in the tissue’. His recommendation was to inject Tensor with Botox even though he had never performed an injection in this area. My ENT’s eyebrows shot straight up when I reiterated what his oral surgeon’s referral had suggested. I also had read an animal research study: the eustachian tube was adversely affected. Botox did not meet Tensor.
Let’s investigate Raphe’s anchor at his ‘Inferior’ attachment – at the bottom on the mandible.
Raphe and the Retromolar Area
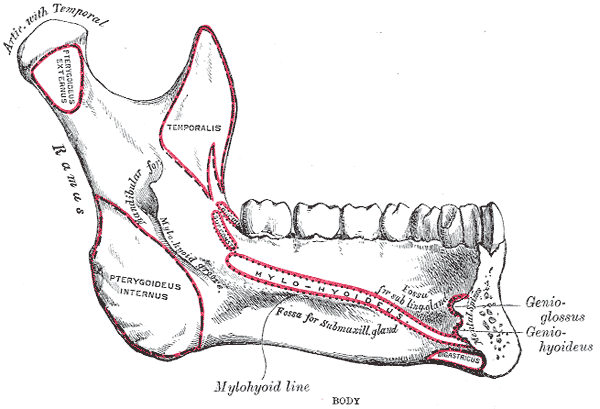
The Pterygomandibular Raphe is located in the retromolar trigone area, a small triangular space behind the third molar. Image from Wikipedia
The Mylohyoid line is a bony ridge on the internal surface of the mandible.
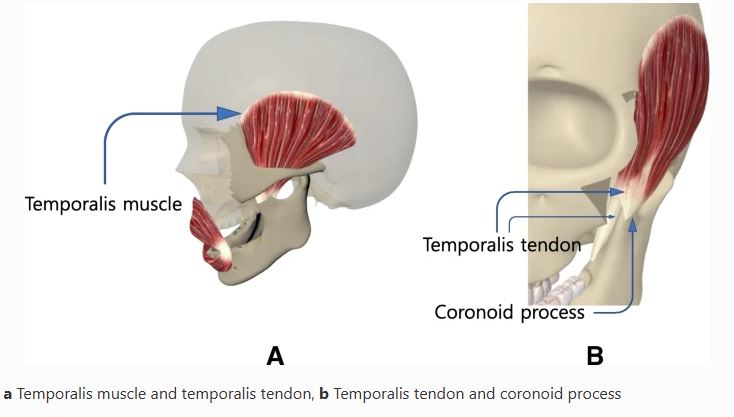
The Temporalis Tendon is a downstairs ‘next-door neighbor’ to Raphe’s anchor behind the third molar (retromolar trigone area). What happens to Raphe’s friend Tempo (temporalis tendon) at the inferior (low) end with Tensor (tensor veli palitini) ‘flopping around‘ in the tissue upstairs?
The tissue in the oropharynx has been ‘assaulted’ by my dentist since October. My mandibular device (NOT mandibular advancement) provokes occlusal shifting which affects the tissue. (This mandibular appliance is gradually providing occlusal stability, which has been destroyed over the years.) Is it coincidence, or cause and effect, that the ‘constrictor muscle’ spasm – initially discovered over a year ago by ENT and both osteopaths – has shifted into the retromolar area – hello Tempo (temporalis tendon).
I wonder if the Temporalis Tendon has suffered consequences from not only Raphe’s orthodontic injury in 1996 but also the TMJ dental mandibular trauma in 1978?
I can answer that in the affirmative based on my recent experiences with my Phoenix Osteopath palpating the temporalis tendon at the coronoid process using Jones Counterstrain techniques to release the ‘triggers’ in the tissue.
Hello ‘Tempo’
Coincidentally, within the last three weeks, my local Osteopath had ventured into my oral cavity. He was most surprised that his previously palpated ‘superior constrictor spasm’ had moved – into the temporalis tendon area. Thus, he began using Jones Counterstrain techniques to release the ‘triggers’ in the tissue.
After having four encounters with Tempo, his fifth exploration revealed Tempo was asleep – no pain, no trigger. This happened today, Friday March 14.
Furthermore, this was the first ‘sharp’ day that wasn’t sharp! Coincidence?
Thank heavens for the palpatory skills of the Osteopaths – imaging shows nothing with these tissue issues. This medical mystery is a clear-cut case of Function…or lack thereof.
We’ve met Tempo and Tensor. Who are Torus (torus tubarius) and Tubby(tubarial salivary gland) …our two remaining ‘superior friends’? They are Tensor’s close neighbors and have been directly affected by Raphe’s trauma.
As mentioned, Tensor (veli palitini) opens the Eustachian tube. A ‘functional’ swallow and yawning activate Tensor in opening this tube.
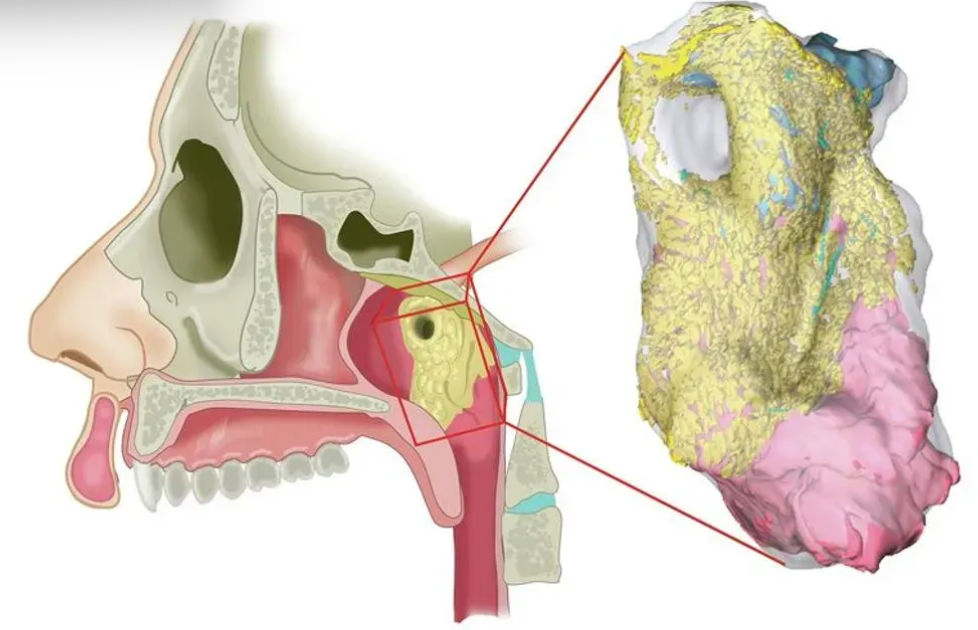
Interactive 3D-reconstruction of histologicl slides.
Schematic reconstruction of the torus tubarius with overlying (tubarial) gland, in its anatomical setting (left) and as 3-D histology reconstruction (right). The glandular tissue is shown in yellow (acini) and ducts (blue).
This dorsomedial view demonstrates the relation of the tubarial gland to the underlying torus tubarius cartilage (dark blue) and muscle (pink).
1- 1977-1981 Dental trauma with TMJ misdiagnosis and mismanagement with MAD (mandibular advancement device*) as well as multiple maxillary dental devices. *Currently, Mandibular Advancement Devices are used to treat sleep apnea. Finding this information months ago was one of several reasons for the development of the this website.
2- 1996 Orthodontic injury causing palate to shift with the left hamular process dropping into the palate. Immediate triggering of fluid in oropharynx with alternating symptom of ‘icepick sharpness’.
3- 1998 —-> 1971 Hamular Process resection to reduce the ‘sharp’ sensation. Symptoms remained. Discovery of an Intubation injury during a sinus surgery (1971) with resulting necrosis (dead bone) in the hamular process region of the palate.
Discovery: The Pterygomandibular Raphe has a superior attachment at the hamulus.
Discovery: The Ptergomandibular Raphe has an inferior attachment in the retromolar trigone area on the mylohyoid line.
Discovery: Tubarial Salivary Glands (2020 discovery) cover the Torus Tubarius at the cartilaginous opening of the Eustachian tube into the oropharynx.
HISTORY and QUESTIONS:
Did the initial insult in 1978 from TMJ mismanagement traumatize the Temporalis Tendon in the retromolar area when the mandible was pulled forward into a Class III malocclusion for four months to ‘recapture the disc’?
The Tensor Veli Palitini ‘flopping around in the tissue‘ was unable to anchor around the Hamulus. There was no hamulus!
Instability of Pterygomandibular Raphe at the superior attachment created damage to this ‘guywire’ Raphe. Did this create dysfunction at the inferior attachment?
Did spasm and tension in the Raphe descend into the inferior attachment area compromising the Temporalis Tendon at the Coronoid Process? Did this create strain on the Temporalis Muscle and thus derange Temporal Bone motion?
Is the puzzling thick fluid since the orthodontic injury generated by the newly discovered (2020) Tubarial Salivary Gland? Is drainage collecting around the Torrus Tubarius as well as tissue folds in the reactive Temporalis Tendon retromolar area?
My recent discovery (Monday, March 10) of the ‘inferior’ attachment of Raphe in the retromolar area adjacent to the Temporalis Tendon triggered innumerable thoughts, swirling and spinning into an ‘aha’ moment of insight – or illusion?
The interaction of the swallow and the tongue at this critical junction (Hamulus / Tensor Veli Palitini / Torus Tubarius / Tubarial Salivary Gland) with the Pterygomadibular Raphe and its attachments has been a missing link in my complex history.
See a larger picture of the Swallow and TMJ involvement (temporomandibular joint) as outlined by Tasha Turzo, DO.
The fact that my Hamular process has been resected along with the recognition of Raphe and friends reaction to this surgery may provide invaluable, overlooked information for anatomical dysfunction/function in the oropharynx that potentially affects physiologic cranial motion via the pterygomandibular raphe – not only through the superior and inferior attachments but also in the interaction with the swallow.
I am most interested to hear the response of my orofacial osteopath to this anatomical information as well as to my wonderings and speculations.
The Medical Power of Light
A NightLase® treatment is commonly used for snoring and sleep apnea. The laser heats the tissue gently and tightens the tissues in the back of the throat. The success rate of NightLase® is up to 85%, usually with three treatments. In my case, tightening the tissue in the throat could potentially address Tensor ‘flopping around in the tissue’ as well as Raphe and his instability.
Dr. Turzo has a clinician trained by Harvey Shiffman, DDS, a leader in dental laser education. She specifically wanted me to benefit from the protocol Dr. Shiffman has created and I had my first treatment on Wednesday, March 8. The treatment was scheduled for 45 minutes; however, mine turned into 90 minutes.
NightLase® stimulated the ‘drainage’ of my fluid. Treatment had to stop multiple times as I dealt with the back of my throat filling up and draining. The last treatment was deep in the back of the throat around the base of the tongue; this stimulated the left side deep drainage from ? (who knows where) and also provoked the taste and the ‘vapor’ that had disappeared during these last few months of treatment. It seemed that the laser light ‘dug’ deep into the tissue in the precise spot where the sharpness lives. The results remain to be seen. Treatments are every 3 – 4 weeks. When I return in April, there will be NightLase® Round 2. The dentist stated that the tightening of the throat tissue will affect my occlusion; in other words, he needs to adjust the mandibular splint after a NightLase® treatment.
There is no doubt that this laser with 1064 and 2049 laser light powerfully affected my symptoms. There are dentists in Phoenix who use NighLase®. Based on my unusual first experience, I only want to have this done in California – with practitioners who have been doing this for several years and can better deal with the ‘unexpected’ and trained by the ‘best.’
And the Waiting Game begins.
I wonder how NightLase® will affect Raphe and friends over time*?
Will Raphe calm down? Will Tensor be able to stop ‘flopping around’ after 30 years? Will Tubby and Torres stop reacting and producing fluid that makes me feel like I’m drowning? Will Tendon stop feeling like a splinter embedded in my throat?