William Garner Sutherland discovered, developed, and taught cranial osteopathy in the mid-1900’s. His discovery, referred to as Osteopathy in the Cranial Field (OCF), was the result of his observations and wonderings while a student at the American School of Osteopathy in 1899.
Sutherland learned well from the founder of Osteopathy, Andrew Taylor Still, who stated that every structure existed because it performed a specific function. Sutherland’s fascination with a disarticulated skull led to his marveling at the complexity of the skull’s architecture.
In an ‘AHA’ moment, he saw the temporal bone was “beveled like the gills of a fish, indicating respiratory motion for an articular mechanism.” Sutherland, 1967, p. 102
Temporal Bone “Beveling”
https://www.headmirror.com/tbone-atlas-anatomy
Finding it impossible to prove that the bones of the cranium did not move, Sutherland discovered that all the articular surfaces in the cranial joints were designed for movement; furthermore, the basic patterns of sutures were the same in every living human. (Sutherland, 1967)
Anatomy textbooks stated that cranial sutures were fused …and unable to move.
THEN and NOW
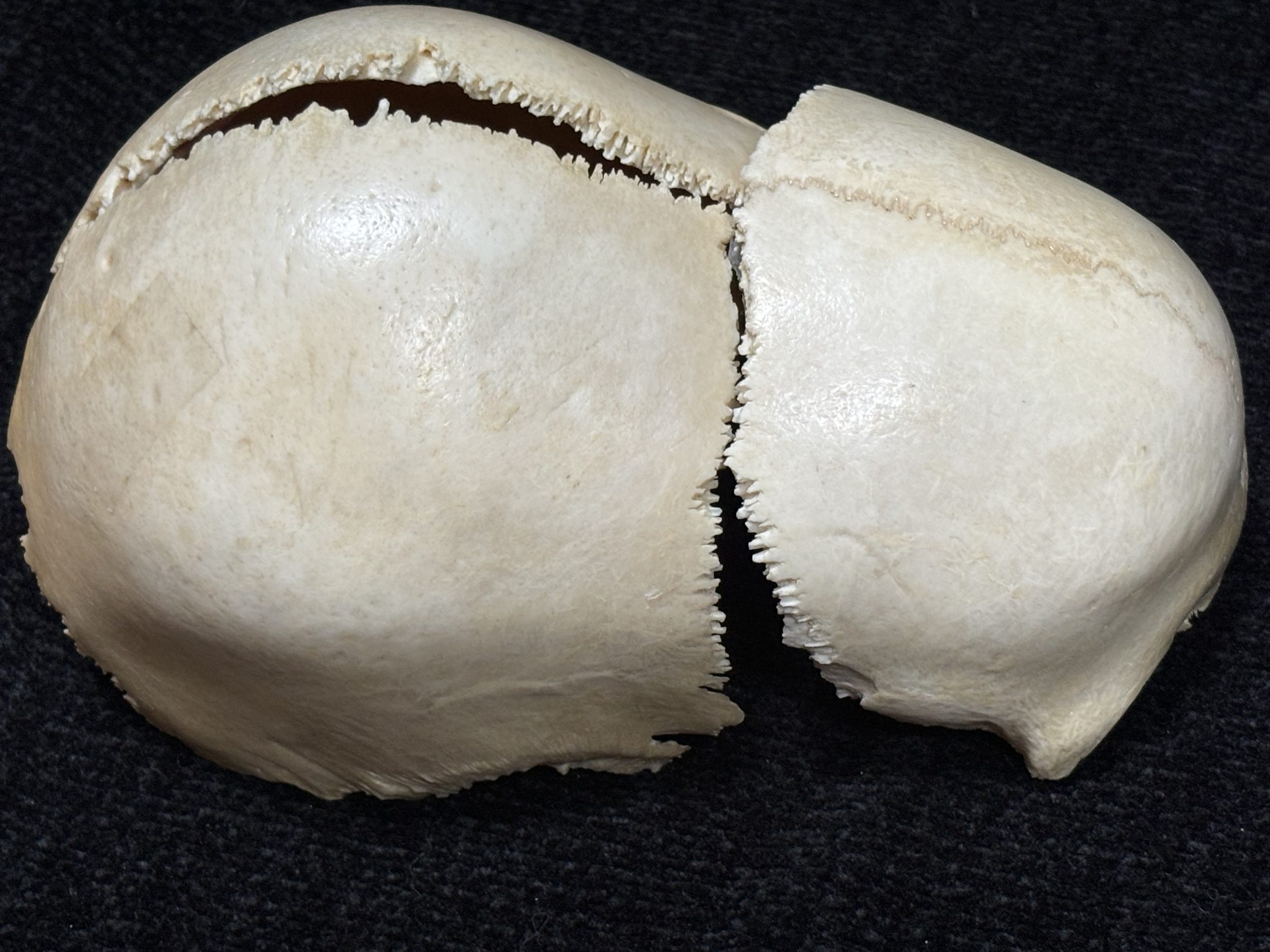
Parietal Bones “Beveling” – interlocking of sutures …intricate ‘puzzle pieces’
cranialconnection.com
Frontal and Parietal “Beveling” – complex articulations
cranialconnection.com
Rather than dismiss his wonderings as foolish, Sutherland became fascinated and was consumed with this idea of movement, integrating the beveling design that he had observed in the skull with his ingrained ‘structure and function‘ education from Still.
Over many years of detailed study of skulls and experimentation on his own head, this ‘consuming’ idea of anatomy became a ‘functional’ reality.
THE HUMAN SKULL
WitmerLab at Ohio University | Ohio University Heritage College of Osteopathic Medicine | www.oucom.ohiou.edu
Dr. Sutherland hypothesized a ‘Primary Respiratory Mechanism’
PRIMARY A system that comes first. This system underlies all of life’s processes, driving bodily functions and giving form and substance to anatomy and physiology.
RESPIRATORY Where does the breath originate? A spark that gives rise to breath that moves through tissues. The foundation of metabolism, enabling exchange between compartments of the body.
MECHANISM Manifesting as motion of the body, driving the interconnectivity of the many parts to create a functional whole that is greater than any of the parts functioning as separate body systems.
SIX COMPONENTS of the PRIMARY RESPIRATORY MECHANISM
1- Cerebrospinal fluid.
2- Intracranial membranes.
3- Articular mobility of the cranial bones.
4- Spinal Cord
5- Intraspinal membranes.
6- The involuntary mobility between the sacrum and the ilia.
The mobility between the cranial bones and between the sacrum and the ilia is not muscular in origin, but rather an involuntary movement that functions as a whole unit during respiration. (Sutherland, 1967)
The heart beats. The lungs breathe. The Central Nervous System (CNS) has involuntary rhythmic motion.
The inherent activity of the CNS, as described by Sutherland, has a ‘respiratory-like motion’ with ‘inhalation’ (expansion) and ‘exhalation’ (contraction) phases.
The subtle motion of the Primary Respiratory Mechanism expresses itself through every cell of the body and influences all bodily functions.
Physicians trained in cranial osteopathy use their hands to perceive (palpate) and facilitate a therapeutic response. Palpatory skills vary with the practitioner and interact directly with the Primary Respiratory Mechanism to balance and integrate the “Whole”, thereby assisting functional integrity and vitality.