Two models illustrate this primary respiratory mechanism: a Mechanical Model and a Pressurestat Model. The dura mater plays a key role in both of these models.
– In the Mechanical Model, the dura serves as a reciprocal tension membrane.
The cranial articulations have no muscular agencies for operation. There is a special membranous tissue that functions as a reciprocal tension membrane limiting the range of the mobility of the cranial. bones. This tension membrane is analogous to the tension spring on the balance wheel of a watch which determines the balance wheel movement. The intracranial membranous tissue accommodates the cranial bone movement during primary respiration. (Sutherland, 1967). An understanding of this intracranial and spinal dural membrane system is mandatory in comprehending the mechanics of this system.
The Dural Membrane
The boundaries of the craniosacral system are the meningeal membranes, specifically the DURAL MEMBRANE.
The dura mater is the outermost of the meninges and is made up of two tightly attached layers except where the venous sinuses are formed. The outer layer of the dura is fused with the internal aspect of the skull as part of the cranial vault. The inner layer of the dura separates from itself at the sinuses and a space is formed for the collection of blood.
(Figure 1) (Upledger, 1983)
The Intracranial Membrane System
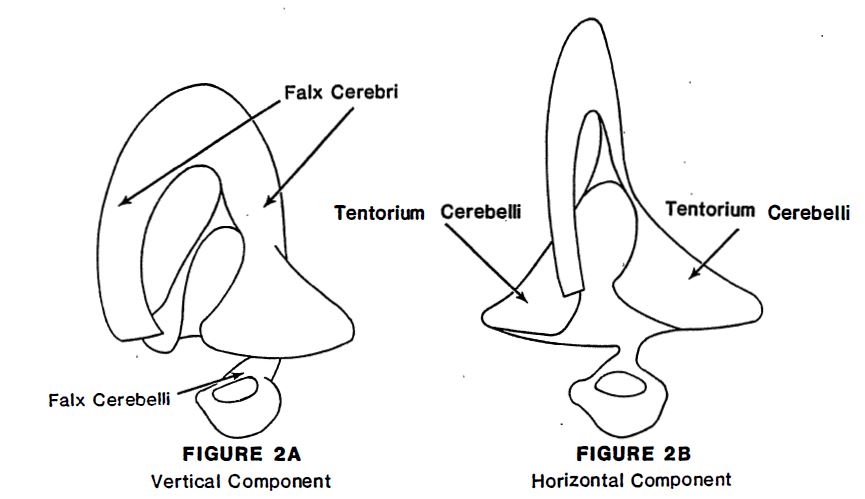
The dura fuses with itself again on the opposite side forming the non-osseous attached INTRACRANIAL DURAL MEMBRANE SYSTEM. This inner layer of the dura is composed of a Vertical Component (the falx cerebri and the falx cerebelll) which separates the hemispheres of the cerebrum and the cerebellum and a Horizontal Component (the tentorium cerebelli) which separates the cerebrum from the cerebellum.
(Figure 2A and Figure 28) (Upledger, 1983)
The Attachments of the Vertical Intracranial Membrane System
The vertical and horizontal components have specific attachments within the cranial cavity. The ATTACHMENTS OF THE VERTICAL MEMBRANE SYSTEM can be viewed in two parts: the falx cerebri attachments and the falx cerebelli attachments.
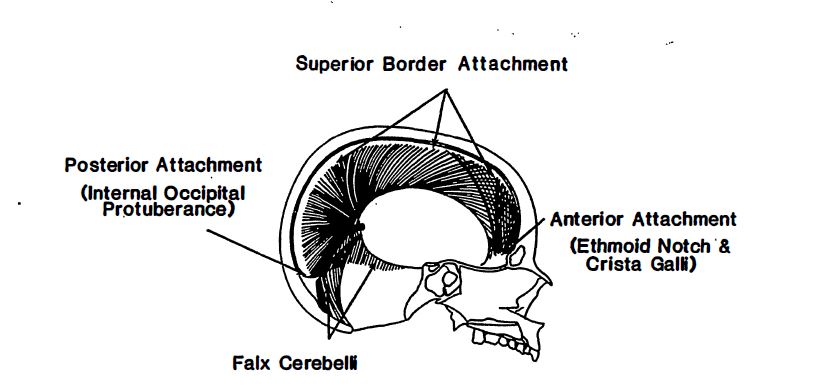
The sickle-shaped falx cerebri separates the cerebral hemispheres. Its superior border is attached to the midline of the skull along the frontal crest underneath the sagittal suture and extends as far posteriorly as the internal occipital protuberance. The inferior border of the falx can be divided into three parts:
1) an anterior attachment to the crista galli of the ethmoid; 2) a middle concave border housing the inferior sagittal sinus; and, 3) a wide attachment to the summit of the tentorium. (Arbuckle, 1977)
Falx Cerebri (Figure 3A) (Upledger, 1983)
The falx cerebelli is formed from the inferior layers of the tentorium cerebelli at a medial position. The falx cerebelli extends inferiorly to the foramen magnum where it encircles this opening in the occiput with a dense fibrous ring.
Falx Cerebelli (Figure 3B) (Upledger, 1983)
The Venous Sinuses
The vertical component of the intracranial membrane system forms the VENOUS SINUSES: the inferior sagittal sinus, the superior sagittal sinus, the straight sinus.
(Figure 4) (Upledger, 1983)
The Attachments of the Horizontal Intracranial Membrane System
The tentorium cerebelli attaches firmly in four places withi the cranium:
– to the clinoid processes of the sphenoid bone – to the petrous ridges and the mastoid portions of the temporal bone – to the posterior angle of the parietal bones – to the transverse ridges of the occiput
These attachments form the HORIZONTAL INTRACRANIAL MEMBRANE SYSTEM. This horizontal intracranial membrane system also forms the venous sinuses.
(Figure 5) (Upledger, 1983)
The Sutherland Fulcrum
The three intracranial membranes (the falx cerebri, the falx cerebelli, and the tentorium cerebelli) are joined together at the straight sinus. The junction at the straight sinus has been called the SUTHERLAND FULCRCM in honor of William Gamer Sutherland. This conceptual model, described as a suspension-automatic-shifting-fulcrum can thus physiologically adapt to postural changes.
(Sutherland, 1967) (Figure 6) (Upledger, 1983)
Dural Tube Continuity
The dura mater connects the occiput with the sacrococcygeal bony complex. As this spinal dural membrane passes through the vertebral canal, it forms a loose sheath for the spinal cord. This spinal dural membrane is an extension of the inner layer of the intracranial dura mater and is referred to as the dural tube. These attachments are of the dura to the bone within the vertebral canal. There are only four areas of osseous attachment in the dural tube:
1) the entire circumference of the foramen magnum, 2) the posterior aspect of the body of the second cervical vertebra, 3) the posterior aspect of the body of the third cervical vertebra and 4) the second sacral segment.
Under normal conditions, movement of the occiput results in movement of the sacrococcygeal bony complex and movement of the sacrococcygeal bony complex produces movement of the occiput Longitudinal gliding is possible due to the relative freedom of movement of the dural tube through the vertebral canal. Thus, restricted motion of the occiput or the sacrococcygeal bony complex can produce symptoms at both ends of the spinal dural mater. The foramen magnum and sacrococcygeal bony complex are functionally connected in a vertical system via the DURAL TUBE CONTINUITY.
(Figure 7) (Upledger, 1983)
Stress Fibers of the Dura Mater
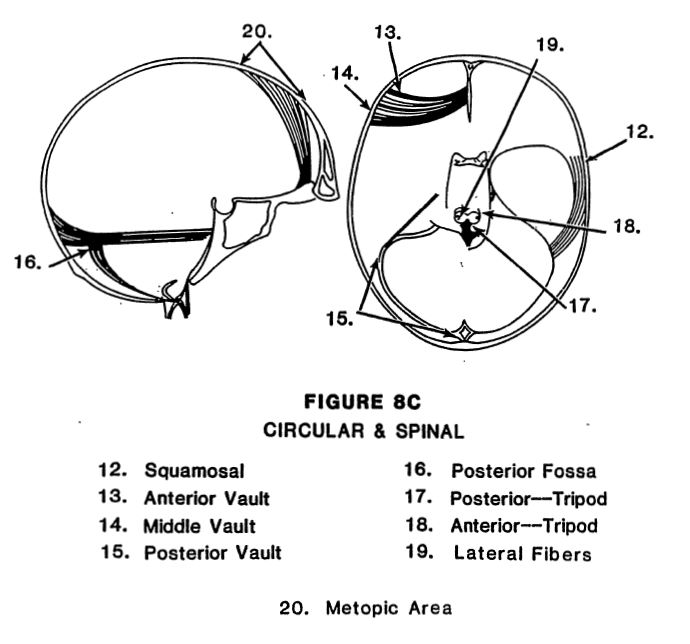
The continuity of the dural membrane within the cranial vault and the vertebral canal can reflect and transmit tensions in many directions. This is further illustrated in the cranium by observing the STRESS FIBERS OF THE DURA MATER. (Arbuckle, 1977) These white fibrous fibers of the dura mater are arranged in definite groupings: 1) horizontal groups; 2) vertical groups; 3) a transverse group; 4) circular groups; and, 5) spinal groups.
Dr. Arbuckle’s book The Selected Writings of Beryl C. Arbuckle, D.O., F.A.C.O.P. (1977) describes these fibrous patterns in detail Even though individual groups of fibers. can be described as having distinct origins and insertions, it must 6e emphasized that this fibrous network is a continuous system.
(Figures 8A, 8B and 8C ) (Arbuckle, 1977)
Abnormal tension in a certain direction over a period of time will cause the fibers of the dural membrane system to malalign. Upledger has observed abnormal fibrous changes in the falx cerebri, tentorium cerebelli, and the falx cerebelli of human and primate cadavers. (1983)